

The built environment mediates our exposure to the outer world, yet how it does so is rarely discussed- probably because there is little credible evidence in the first place on how exactly actions in the built environment affect health, nutrition, or other spheres of life. How should such a conversation begin? The work that ARCHIVE does in low- and middle-income countries, using interventions in the built environment to improve people’s health, provides a useful starting point. For instance, ARCHIVE’s ongoing initiative to reduce pathogen contamination and transmission by improving floor surfaces from dirt to concrete offers a relevant case in point: floors are a potentially important source of contamination for infants and young children who spend a lot of time sitting and playing on the floor, especially before they start walking. These children are also most vulnerable to repeated or chronic infections and related malnutrition and are at greater risk of mortality from such causes than adults. But does floor surface improvement work? How can we create evidence that is acceptable to the scientific community that is an intervention worth supporting? Here are some ideas to this end.
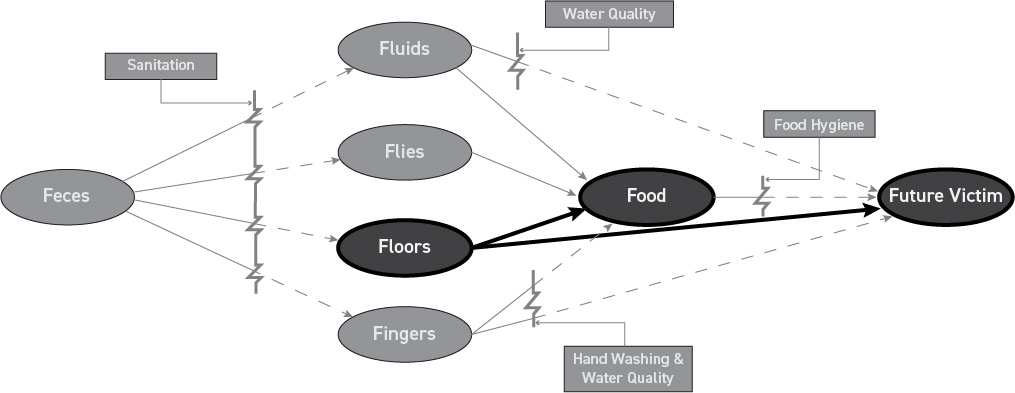
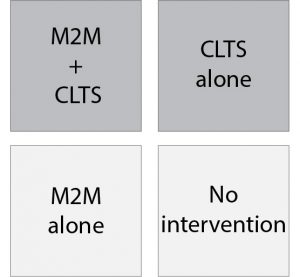
The fact is that the effectiveness of interventions to the built environment in reducing pathogen infestations and diarrheal diseases under real-life conditions is challenging to prove. Pathogens may be transmitted in a myriad of other ways – via flies, animal feces, stagnant waters – and any of those may cancel the gains made by floor surface improvements (see figure 1). Children will still get sick and people will conclude that the change from mud to mortar had no effect. To overcome that, efforts at controlling pathogen transmission should target the peri-domestic areas as well and eliminate those pathogens from the wider environment so that they have fewer chances of eventually entering the home. This notion could usefully be paired to “community-led total sanitation” (CLTS), an approach developed and used in Bangladesh to improve hygiene practices by changing the behavior of entire communities at a time. CLTS seems to have been successful in reducing perennial problems like open defecation but there is still a lot of diarrhea in Bangladesh, so there has to be space for additional actions. Floor surface improvements may be one of them. One way to test the added value of floor surface improvements would be to design a trial where randomly selected communities receive CLTS alone, and other communities receive CLTS in combination with ARCHIVE’s Mud to Mortar (M2M) intervention (where a dirt floor is replaced with a concrete assembly). Doing so would offer the option for a full community randomized control trial, a design that is perfectly acceptable on scientific grounds. The proposed 2×2 factorial design (see figure 2) would compare:
a) villages that receive CLTS and M2M
b) villages that receive only CLTS
c) villages that receive only M2M
d) villages that receive neither interventions
Provided that the number of villages in each cell is statistically sufficient to support the hypothesis, such a study would adequately inform whether M2M has any additional effect on top of CLTS, whether M2M alone has an effect compared to controls, and whether CLTS has any effect compared to control Scientists would love it.
ARCHIVE, now a credible organization, is ideally positioned to advance this prospect. Using its platform, it could aim at validating the role of design in global health by creating an evidence base showing the effectiveness of interventions in the built environment on public health. To make it convincing to donors, the study should involve reputed researchers from all relevant fields (biologists, implementation scientists, behaviorists) to accompany the proposal development and the implementation phases. Bringing the model to fruition and documenting it carefully would be of great service to the design profession, to public health, and to the ultimate beneficiaries.

Gilles Bergeron, PhD. | Senior Vice President, the New York Academy of Sciences